
CHA position paper calls for default benefit for Hospital in the home
June 19, 2026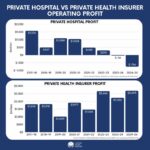
Insurers profiting while hospitals struggle: New data
June 22, 2026
Opinion

Poor mental health is no longer a private misfortune. Its costs cascade onto hospitals, employers and public budgets. The OECD’s 2026 report The Economic Case for Preventing Mental Ill Health estimates that mental ill health will cut GDP across European economies by an average of 1.7% a year through to 2050, driven largely by lost productivity. Australia is not exempt; if anything, our geography compounds the problem.
The OECD’s lesson is twofold. Prevention and early intervention are among the highest-return investments available — many are cost-effective, and some save money. Yet those gains routinely go unrealised, because good interventions are rarely delivered at scale. The problem is not only what we fund, but whether the system can actually reach the people who need it.
Australia is not short of architecture. Under the National Mental Health and Suicide Prevention Agreement and its Evaluation Framework, governments have committed to a national evaluation culture in which evidence guides where money is spent. Yet a stubborn treatment gap remains, and it falls hardest on regional, rural and remote communities, where out-of-pocket costs, thin specialist coverage and workforce shortages mean long wait times, or no service at all.
Nowhere is this clearer than in inpatient psychiatry. Too few psychiatrists will take on inpatient work, leaving acute services in regional areas dangerously under-resourced. Medicare does not adequately remunerate it, and many psychiatrists now prefer office-based or telehealth practice to the round-the-clock responsibility of holding patients under their bed card. Several private facilities have already closed because they could not attract them.
Yet there are models that already point the way. At Cabrini Health’s Lisa Thurin Women’s Health Centre — Australia’s first women-only mental health hospital — published outcomes are striking: of more than 1,000 women admitted over three years, 93% rated their care as excellent and 95% felt safe. When psychiatrists alone could not staff the unit, the service built a shared-care model in which specialist GPs managed admitted patients under psychiatrist supervision. It worked — strong clinical outcomes, and GPs eager to take part. This is exactly the kind of team-based, full-scope model Australia should be funding and scaling, not improvising in a crisis. The only thing that undercut it was the money: because Medicare rebates GPs so poorly for inpatient work, patients faced gaps of $1,000 to $1,500 per admission while psychiatrist-led stays carried none. This pushed people to choose based on cost rather than clinical need.
So what should change? In the short term, uplift Medicare funding for inpatient work, for psychiatrists and for the specialist GPs and, in time, nurse practitioners who can safely share that care under supervision, so inpatient work is no longer the least attractive option on a roster, and so effective shared-care teams are no longer penalised with patient gaps. But a fee uplift is a bridge, not a destination. It should be the first step toward outcomes-based funding that rewards retention, team-based care and patient outcomes rather than throughput: the model that would let services like Cabrini’s be properly resourced and replicated in areas that need it most.
Alongside this, the “area of need” classifications applied to regional Australia should be reviewed to reflect actual demand, with a dedicated allocation of psychiatrists — including overseas-trained doctors, who are often keener on inpatient work — as a feasible interim measure.
Australia has already committed to let evidence decide where investment goes. On inpatient psychiatry, the evidence is in. Acting on it by prioritising workforce incentives is how we keep the system standing.
Annabelle Wang
Annabelle brings consulting experience across government, health and aged care, a strong public health background, and a passion for policy that leads to more equitable health outcomes for all Australians.
Related posts
