
The Catholic sector should lead on AI, together
June 18, 2026
NDIS reforms risk cutting off vulnerable Australians before alternatives exist
June 18, 2026
Opinion

By Dr Katharine Bassett
Catholic Health Australia Director of Health Policy
Every day in this country, someone walks into a public hospital emergency department frightened, in pain, and entirely at the mercy of whatever system happens to receive them. They do not ask who runs the hospital. They do not care whether it is operated by the government or a Catholic health ministry that has been caring for the sick since before Federation. They care only that someone sees them, and sees them quickly, and treats them as though they matter.
In a not-for-profit Catholic hospital, every patient matters. They are not simply units of activity or weighted separations or line items in a bilateral funding agreement, but persons possessed of an inherent and inviolable dignity. Catholic Social Teaching has a phrase for the organising principle that follows from this conviction: the common good, the conditions under which every person, and particularly the most vulnerable, can flourish. It is a vision of healthcare not merely as a transaction between provider and patient, but as a contribution to the community of which both are part.
That principle has guided Catholic healthcare in Australia for more than 150 years. Long before Medicare, long before the National Health Reform Agreement, long before anyone in Canberra had heard the phrase “activity-based funding,” religious sisters were establishing hospitals in communities that no one had any interest in serving. They did it with minimal resources and maximum resolve. And the institutions they built endured as serious, complex, modern health services that today operate emergency departments, train the next generation of doctors, and deliver some of the most acute care in the country. They do so, it should be noted, under state service agreements that often fund them below the National Efficient Price, ultimately delivering public hospital care at a discount.
What has not been widely understood, until now, is just how well they do it.
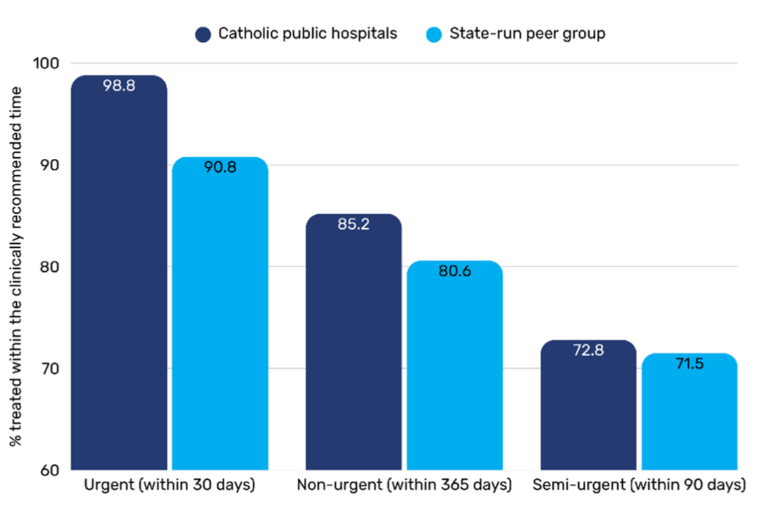
Across all urgency categories, Catholic public hospitals are outperforming their state-run peers. For urgent surgery, 99 per cent of patients receive their operation within the clinically recommended window, compared with 91 per cent in peer hospitals. For non-urgent procedures, the median wait at a Catholic public hospital is 178 days; at a comparable state-run facility, it is 257. That is 79 days of someone’s life returned to them. These are extraordinary results that deserve to be highlighted.
Weighted average proportion of patients receiving surgery within recommended time, by urgency category
Median wait times for elective surgery
| Urgency category | Catholic public hospitals | State-run peer hospitals |
|---|---|---|
| Urgent | 12 days | 14 days |
| Semi-urgent | 62 days | 63 days |
| Non-urgent | 178 days | 257 days |
Source: Australian Institute of Health and Welfare MyHospitals dataset, 2024–25
The instinct in Australian policy circles is to explain such findings through the language of management: better systems, leaner processes, smarter rostering. And no doubt those things play a role. But they are not sufficient as an explanation, because they do not account for the animating purpose beneath them. Catholic hospitals do not pursue efficiency as an end in itself. They pursue it because every dollar wasted is a dollar that could have been spent on a patient, and every unnecessary day on a waiting list is a day of suffering that a person should not have to endure.
There is a theological word for this that has become unfashionable in policy circles, which is precisely why it needs recovering: vocation. The staff who work in Catholic hospitals, many of them not Catholic and some not religious at all, participate in institutions that understand their work as a calling. Every public hospital in this country is full of dedicated people who entered healthcare to help others. State-run hospitals face enormous pressures of their own, including governance structures they did not design, funding models that reward activity over outcomes, and political cycles that rarely align with what patients need. The difference is not in the compassion of the staff, but in what the system around them is designed to prioritise. It is what happens when, alongside the necessary question ‘have we met the benchmark?’ an institution also insists on a second one: ‘have we done right by this person?’. The remarkable thing the data shows is that the second question, pursued seriously, tends to produce better answers to the first. Vocation, in this sense, is not a private spirituality. It is a commitment to be the kind of institution a community can rely on, and one whose failure would be felt as a loss far beyond its walls.
There is a deeper point here that the current policy conversation is not yet equipped to hear but needs to. Australia is in the early stages of a reckoning with the cost and sustainability of its care economy. Health, aged care, and disability are areas of public expenditure that will define the fiscal character of the next generation. Policy makers are all asking the same question: how do we get more value from the system?
It is the right question. But value is not merely a fiscal concept. A system that is cheap but cruel is not efficient. Efficiency that loses sight of the patient at its centre is not, in the end, efficiency at all. The distinctive contribution of Catholic healthcare, and the reason its performance data should command attention rather than polite surprise, is that it demonstrates something the utilitarian imagination struggles to credit: that an institution animated by love of neighbour can match and often outperform institutions with far greater resources and the full weight of the state behind them. Not always. Not in every metric. But consistently enough, and by margins large enough, that the finding cannot be dismissed as coincidence or selection bias.
The people we are talking about here are the woman in Fitzroy whose cancer surgery happened two weeks after diagnosis rather than two months. They are the elderly man in Newcastle whose urgent procedure was completed on time because the hospital that received him has a culture that treats timeliness as a moral obligation, not a KPI. They are the young mother in Werribee whose emergency presentation was met not only with clinical competence but with the kind of attentiveness that says: you are why we are here.
Somewhere in Australia today, a patient will be added to an elective surgery waiting list. At some hospitals, they will wait almost nine months. At a Catholic public hospital, on average, they will wait nearly three months less. No one who has lived through that difference would call it marginal. No government that has seen the evidence should either.
Catholic public hospitals have long been asked to do more with less, and the evidence shows they have risen to that challenge. But excellence achieved under strain is not the same as excellence sustained. A system that leans on the goodwill of mission-driven organisations without funding them fairly is a system that has been lucky. And luck is not a health policy.
Australia will need every good idea it can find to build a health system worthy of its people and the communities that hold them. The Catholic sector has shown what is possible when care is treated as a vocation rather than a transaction. The least the system can do is fund that work fairly. The smartest thing it could do is learn from it.
Dr Katharine Bassett
Katharine is a respected leader committed to sparking positive change and reforming Australia’s health system. She has nearly a decade of experience developing evidence-based solutions to Australia’s biggest health and social policy challenges.
Related posts
